
Let me be upfront from the start — I'm a man, and menopause is something I'll fortunately never experience personally. But I've coached dozens of women between 45 and 55 who are living exactly these experiences, asking exactly these questions, and who deserve real answers rather than vague generalities or recycled myths. This article is everything I tell them in sessions, put in writing. For you.

Menopause navigated well. This is not the exception — it's what becomes possible when you understand what's happening and act accordingly.
Because menopause is not a disease. It's a biological transition — powerful, sometimes brutal, but navigable. And what you've done over the past ten years in terms of exercise, nutrition and sleep will reflect directly in the severity of what you're experiencing now. Yes, really. But here's what matters: it's never too late. The right habits adopted today can reverse or significantly attenuate the effects — at any stage.
Perimenopause or menopause — where are you exactly?
A clarification that changes everything — because many women don't realise they're already in perimenopause, sometimes for several years. Perimenopause is the transition phase that precedes official menopause, typically between ages 42 and 51. Hormones begin to fluctuate, cycles become irregular, and the first symptoms appear. Menopause itself is technically diagnosed after 12 consecutive months without a period.
Why does this matter? Because the strategies to implement apply from perimenopause onwards — or even before. Waiting for "official" menopause to act means losing several precious years when interventions have the greatest impact.
Timeline reference
Perimenopause: average age 42-51, lasts 4-10 years · Menopause: 12 months without a period, average age 51 · Post-menopause: the rest of life · The transition often begins well before the first obvious signs — today's habits count.
The full hormonal picture — what's actually happening
Oestrogen gets all the attention during menopause — as if it were the only hormone involved. In reality, it's an entire orchestra going out of tune. Understanding each instrument helps you respond more effectively.
Oestrogen — the conductor taking retirement
Oestrogens (primarily oestradiol) are produced by the ovaries and play a role in almost everything: temperature regulation (hence hot flushes when they decline), bone density, cardiovascular health, collagen production in skin and fascia, mood, memory, mucosal lubrication, and insulin sensitivity. When they drop — and they drop fast — the effect is systemic.
The decline is not linear: during perimenopause, levels fluctuate erratically — sometimes very high, sometimes very low — before stabilising at a permanently lower level after menopause. These fluctuations explain the emotional instability and unpredictable symptoms of this period.
Progesterone — the first to leave
Less discussed but equally important: progesterone often drops before oestrogen, in early perimenopause. Its role: balancing the effects of oestrogen, promoting deep sleep, reducing anxiety, supporting the thyroid. Its decline explains the sleep disturbances, irritability and early weight gain that appear before hot flushes even begin.
Testosterone — yes, women need it
Surprise? Women produce testosterone — roughly 10 times less than men, but it's just as essential. It supports muscle mass, bone density, libido, energy, confidence and athletic recovery. During menopause, testosterone levels drop by approximately 50% compared to the peak of the 20s. This decline is often the underestimated cause of chronic fatigue, loss of motivation and the difficulty maintaining muscle after 45.
The good news? This is precisely where strength training with free weights makes its mark. Squats, deadlifts and lunges trigger an acute testosterone release — intensity and large muscle groups are the key triggers. Long-term, regular resistance training improves sensitivity to androgen receptors, making the testosterone that's still available more effective.
Cortisol — the intruder that exploits the chaos
When oestrogen and progesterone decline, cortisol — the stress hormone — loses its previous modulation. Result: everyday stress produces a more intense cortisol response. Chronically elevated cortisol equals accelerated abdominal fat storage, plus muscle breakdown, poor sleep, and insulin resistance. This is the infernal triangle of menopause — and many women never connect their belly changes directly to their stress levels.
Insulin — declining sensitivity
Oestrogens played a protective role on insulin sensitivity. Without them, cells become progressively more resistant — glucose accumulates in the blood, insulin rises, fat stores more easily. This is why women who never had weight problems see their waistline change after 50 despite an identical diet. It's not willpower. It's biochemistry.
Symptoms — including the ones nobody connects to menopause
Hot flushes and night sweats — everyone knows those. But there's a whole list of symptoms women don't spontaneously associate with menopause — yet they're directly linked to hormonal decline.
Hot flushes & night sweats
The classic. Declining oestrogen disrupts the hypothalamic thermostat. Affects 75% of women to varying degrees.
Sleep disturbances
Progesterone decline + night sweats + elevated cortisol. Deep sleep fragments — and less deep sleep means less HGH means slower recovery. A vicious cycle.
Abdominal fat gain
Insulin resistance + elevated cortisol + muscle loss. Same eating, same calories — the body redistributes fat differently.
Muscle mass loss
Testosterone decline + reduced HGH + insulin resistance. Without active intervention, 1-2% of muscle mass is lost per year after 50.
Joint pain & stiffness
Less known: oestrogens have anti-inflammatory properties. Their decline increases systemic inflammation. Less elastic fascia, more fragile tendons.
Brain fog & memory
Oestradiol plays a neuroprotective role. Its decline affects concentration, short-term memory and mental clarity. "I'm losing my mind" — no, it's hormonal.
Mood swings & anxiety
Hormonal fluctuations in perimenopause directly affect serotonin and dopamine. Not weakness — chemistry.
Urinary problems & prolapse
Often the most taboo. Yet directly linked to menopause — covered in detail below.
Fascia, collagen & hydration — menopause from the inside
Oestrogens directly stimulate collagen production. Their decline leads to a loss of approximately 30% of collagen in the first five years of menopause. In practice: less elastic and hydrated fascia, skin that loses firmness, more painful joints, more fragile tendons, reduced mobility. The morning stiffness many women describe after 50? That's often this.

The fascial network — rich in collagen, directly affected by the decline of oestrogens. Elasticity, hydration and targeted nutrition make a real difference.
Cellular hydration & fascia — busting the salt myth
Fascia is approximately 70% water. But water alone is not enough — it needs minerals and electrolytes to be retained and used in tissues. And here's where we need to demolish a persistent myth: not "salt makes you thirsty" — but "salt is bad for you". This is fundamentally wrong. Refined industrial white salt — pure sodium chloride, bleached, devoid of minerals — yes, avoid it. But Guérande sea salt (unrefined grey sea salt) is an entirely different matter.
Guérande salt, harvested artisanally without additives or chemical processing, naturally contains magnesium, potassium, calcium, zinc and dozens of trace elements. Its mineral composition is close to that of bodily fluids — making it directly bioavailable. These electrolytes are the keys that allow water to cross the cell membrane and genuinely hydrate cells and fascia.
Patrik's protip — cellular and fascial hydration
A small pinch of Guérande salt in your morning glass of water (with lemon juice if you like). One of the simplest and most impactful habits for fascial, joint and skin hydration — particularly after menopause where tissue dehydration accelerates. Clients who apply this advice drink less, visit the bathroom less often, and report improved joint mobility within weeks. This isn't "eating salty" — it's remineralising. Replace all refined white salt with Guérande salt in all your cooking.
The pelvic floor — the topic nobody discusses
Gently but directly — because this is too important to skip.
The pelvic floor is a group of muscles and ligaments that literally supports your internal organs: bladder, uterus, rectum. It's maintained by collagen and connective tissue. You've guessed what follows: when oestrogens decline, this collagen weakens. The pelvic floor loses tone and resilience.
The concrete consequences range from stress urinary incontinence (coughing, laughing, jumping) to pelvic prolapse — when organs descend into the pelvic cavity for lack of sufficient support. A sensation of pressure, of heaviness low in the abdomen, the impression that "something is descending". A problem affecting up to 50% of women at some point in their lives, often aggravated by menopause and frequently under-diagnosed or minimised.
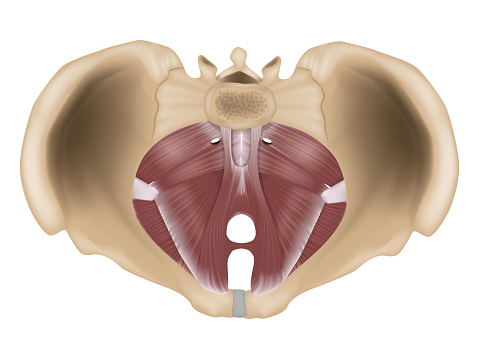
The pelvic floor supports the bladder, uterus and rectum. Oestrogen decline weakens the supporting ligaments — which is why actively working this muscle group matters.
The good news? A strong pelvic floor is trainable. And this work integrates into every workout.
Integrating pelvic floor awareness into every exercise
The first step is awareness — and it's simpler than it seems. The pelvic floor contracts upward and inward (as if trying to stop the flow of urine). Learn to feel this contraction, then to release it. Both matter — an over-contracted pelvic floor creates as many problems as an under-contracted one. In practice: on a squat or deadlift, a gentle pelvic floor activation before the push protects and strengthens simultaneously. On every exertion: exhale, engage the floor, push. Not a separate session — a consciousness to integrate.
Specific pelvic floor exercises
Classic Kegel: 5-second contraction, 5-second release. 3 sets of 10. Anywhere, anytime. · Rapid Kegels: Short contractions (1 sec) × 20. Stimulates the fast-twitch fibres essential against effort incontinence. · Glute bridge with engagement: On the way up, exhale and contract the pelvic floor. On the way down, fully release. · Deep squat held: Maintained low position 30-60 seconds — one of the best exercises for pelvic floor mobility and opening.
What you're doing wrong — the mistakes that make everything worse
Many women make the following mistakes with the best intentions in the world — not out of ignorance but for lack of information adapted to their hormonal reality.
Cardio only, without preparation or strength training
Running is excellent — but exclusive, prolonged cardio without progressive preparation and complementary strength work raises cortisol durably and promotes muscle loss. A marathon or trail run prepared over months with adequate nutrition and strength training is completely fine. The problem is not running — it's the absence of preparation and balance.
Eating less to lose weight
Chronic caloric restriction signals famine to an already stressed body. Result: slower metabolism, elevated cortisol, muscle loss, and weight regain at the slightest caloric increase. The problem isn't calories — it's insulin and body composition.
Avoiding strength training "to not bulk up"
The myth of the woman who gets "too muscular" with weights. Without testosterone in quantity, significant muscle volume is almost impossible. What strength training actually does: burns fat, firms, improves posture, boosts hormones. Exactly what you need.
Gym machines only
Machines isolate one muscle in a fixed plane. They don't engage stabilisers, don't trigger the same hormonal response as free movements, and don't work the pelvic floor or global coordination. For menopausal women, it's the bare minimum.
Stopping heavy lifting "because of joints"
Inverted logic. Tendons and joints need load to maintain themselves. Progressive resistance training stimulates collagen production in tendons and increases bone density. Avoiding it accelerates degradation — not the reverse.
Neglecting sleep "because there's no time"
70% of HGH — the primary anti-ageing hormone — is produced during deep sleep. In menopause, this sleep is already compromised. Sacrificing it further cuts the last available thread of hormonal recovery.
The most heard sentence — and the most counter-productive
"I eat less than before and I'm still gaining weight." This is real — and it's not a willpower issue. It's hormonal biochemistry. The answer isn't eating even less. It's eating differently (fewer fast carbs, more protein), moving differently (strength training, not just cardio) and sleeping seriously. The solution is hormonal, not caloric.
Sport — what actually works
Free weight strength training — the most valuable investment
Studies published in 2024-2025 confirm: resistance training preserves strength, balance and body composition throughout the menopausal transition — at any phase. Free multi-joint exercises — squat, deadlift, lunges, pull-ups, press — are incomparably more effective than guided machines for hormonal response.
But strength training alone isn't enough. What genuinely transforms the body in menopause is the combination of strength + movement + mobility — in three dimensions. Complex movements integrating rotations, changes of direction, carries, and multi-plane challenges engage the nervous system, deep muscle chains, the pelvic floor and global coordination far more richly than any static plank. Core and pelvic floor work significantly more in dynamic 3D movement than in fixed positions. Posture improves. Joints stay healthy. And it's genuinely enjoyable rather than a punishment.
Specific adaptations for menopause
- Priority to the lower body
Squats, deadlifts, lunges, hip thrusts — the largest muscle groups. Maximise hormonal response, protect hip bone density (critical for osteoporosis) and strengthen the deep abdominal stabilisers.
- Extend recovery between sessions
Recovery time increases with menopause — repair hormones are less abundant. 48-72 hours between intense strength sessions is recommended. Better to have 3 well-recovered sessions than 5 exhausting ones.
- Moderate to heavy loads
60-80% of maximum (8-12 repetitions). Heavy enough to trigger the hormonal response, not so heavy that technique breaks down. Progression must be gradual — tendons and ligaments adapt more slowly than muscles.
- Pelvic floor integration — every session
On every exertion: exhale, engage the pelvic floor, execute the movement. This awareness simultaneously protects and strengthens. Not a separate exercise — a consciousness to develop.
- HIIT — maximum twice a week
HIIT is excellent for insulin sensitivity and HGH stimulation. But in menopause, too much HIIT raises cortisol. 2 sessions of 20-25 minutes per week is the sweet spot.
- Movement Training — at least once a week
Complex 3D movements, rotations, free bodyweight, mobility. Varies the sessions: never do exactly the same thing twice. The body adapts best to varied stimuli.
Exercises that boost testosterone in women
Weighted squat
Studies show 15-30% testosterone increases above baseline after heavy squats. The peak occurs 15-30 minutes post-training. Goblet squat (kettlebell at chest) is the ideal entry point.
Deadlift
Engages almost every muscle in the body. Massive hormonal stimulation — testosterone and HGH. Loads the spine and hips — exactly where bone density is at stake. Learn with a coach, then practise regularly.
Lunges and hip thrusts
Target glutes and hamstrings. Hip thrusts activate glutes at 100% and are particularly recommended for post-menopausal women for their lumbar protection.
Pull-ups and rows
Upper body pulling work. Back, biceps, shoulders. Free pulling movements complement the overall hormonal response. Pull-ups (with elastic assistance if needed) are among the most functional exercises available.
Short sprints
20-30 seconds of maximal effort. Very significant testosterone and HGH response. Practise with moderation (cortisol) — twice a week is plenty.
Multi-joint circuit
Squat + row + lunge + press in sequence without long rest maintains high lactic acidosis and intense hormonal signal throughout the session. Efficient and time-effective.
Nutrition — eating for your hormones, not against your scales
Protein — your number one priority
With accelerated muscle loss in menopause, protein becomes non-negotiable. Requirements increase — 1.5 to 2g per kg of body weight per day is a realistic target. Meat, fish, eggs, legumes, cheeses. At every meal, not just dinner. The first thing to eat after breaking a fast? Protein.
Carbohydrates — not the enemy, but choose wisely
Refined carbohydrates (white bread, pasta, sweets, juice) create insulin spikes that, in menopause where insulin sensitivity is already degraded, store directly as abdominal fat. Complex carbohydrates (root vegetables, legumes, whole grains, whole fruits) maintain stable blood sugar. Not zero carbs — the right carbs, at the right time.
Healthy fats — and no, they don't make you fat
Let's be clear: fat doesn't make you fat. What makes you fat is insulin — and insulin rises with fast carbohydrates, not with fat. Sex hormones are made from cholesterol. Without sufficient dietary fat, hormonal production collapses further. Avocado, olive oil, oily fish (salmon, sardines, mackerel), nuts, eggs. Your hormonal allies.
Dietary collagen — for fascia and joints
Facing a 30% collagen loss in 5 years, dietary intake of collagen precursors becomes important. Bone broth — long simmered with cartilage and ligaments — is the most bioavailable source. Whole fish with skin. Eggs. Vitamin C in generous quantities (peppers, kiwis, citrus) — it's essential for collagen synthesis.
Intermittent fasting & menopause — busting the myth
The idea that intermittent fasting is "dangerous" or "contraindicated" for menopausal women is — to put it politely — poorly informed. This warning comes from studies on premenopausal women of reproductive age, where prolonged fasting can occasionally affect reproductive cycles. After menopause, the situation changes completely.
A 2022 study on the 16:8 protocol in menopausal women showed: loss of body fat, improved body composition, no negative effects on reproductive hormones or bone density. Reproductive hormones are stabilised — they no longer fluctuate with the cycle. The body tolerates fasting very well.
And recall: intermittent fasting boosts HGH production by up to 2,000%. HGH — human growth hormone, the one that regenerates your body, preserves muscle and keeps you biologically young. More HGH is almost always beneficial — and fasting is the most powerful natural lever to stimulate it.
The next time you encounter content claiming fasting is harmful for women — ask who wrote it, whether they read the studies, or whether they repeated information seen elsewhere without verification. Health information travels fast on social media — but it doesn't always age well when it hasn't been fact-checked. The studies exist, they're serious, and they say the opposite.
Natural supplements — the documented trio
Magnesium — the mineral almost everyone is deficient in
Magnesium is involved in over 300 biochemical reactions: sleep regulation, stress management (cortisol reduction), muscle function, bone health, hormonal balance. In menopause, requirements increase and intake is often insufficient. Magnesium glycinate or bisglycinate (300-400mg in the evening) — the best absorbed form, without laxative effect. Food sources: pumpkin seeds (one of the most concentrated sources), wheat bran, cashews, almonds, nuts, dark chocolate, legumes, buckwheat.
Omega-3 — anti-inflammatory and neuroprotective
Oestrogens had anti-inflammatory properties. Their decline increases systemic inflammation — joint pain, brain fog, mood instability. Omega-3s (EPA/DHA) partially compensate for this lost anti-inflammatory effect. 1-2g of EPA/DHA per day — fish oil or algae oil. Important note on flaxseed and camelina oil: these are rich in ALA (plant omega-3) and excellent for rebalancing the omega-6/omega-3 ratio. But conversion from ALA to active EPA and DHA is limited (0-9% according to studies) — they don't replace oily fish for documented anti-inflammatory effects. Use them in cooking (cold, never heated), but ensure you have direct sources of EPA/DHA. Food sources: salmon, sardines, mackerel, herring — 2-3 times per week.
Vitamin D3 + K2 — the bone and hormone duo
Vitamin D is technically a precursor hormone. It plays a role in sex hormone synthesis, bone health, immunity and mood regulation. Most people in Switzerland are deficient in autumn and winter. In menopause where osteoporosis becomes a real concern, this is non-negotiable. 2,000-4,000 IU of D3 with K2 (MK7, 100-200mcg) to direct calcium to bones rather than arteries. Check your blood level once a year. And natural light is mandatory — a daily outdoor outing even in grey weather, and a day in the mountains or on the ski slopes is one of the best natural vitamin D boosts available. Exposing your forearms during the lunch break when weather allows — 15 minutes suffices.
A word on creatine — with caution
Creatine is much discussed for menopause, and studies are promising for muscle mass and cognition. But here's what's often omitted: creatine rapidly increases strength and muscular water retention — but tendons and ligaments adapt much more slowly than muscles. This creates a real risk of tendon overload and inflammation, particularly in people who aren't yet training regularly. Muscle spasms have also been reported. Regular supplementation also leads to reduced endogenous creatine production — the body produces less because it receives some externally. My recommendation: stimulate natural creatine production through diet and training. Rich food sources: red meat, salmon, herring, sardines, tuna. And heavy resistance training directly stimulates the creatine-phosphocreatine cycle in muscle.
Daily habits — the routine that changes everything
Sleep — the absolute priority
Bed before 11pm, cold dark room
- Bed before 11pm — the HGH peak occurs between 11pm and 2am. In menopause where HGH is already reduced, every nocturnal peak counts.
- Bedroom at 18-19°C — hot flushes are worsened by ambient heat. A cool room directly improves sleep quality.
- No screens 60 minutes before bed — blue light suppresses melatonin, already less well-regulated in menopause.
- Magnesium glycinate in the evening — promotes deep sleep and reduces nocturnal cortisol.
Earthing & natural light
Reconnecting the body to its natural environment
- Natural light within 30 minutes of waking — synchronises the circadian clock, regulates morning cortisol and prepares evening melatonin.
- Regular earthing — barefoot on grass, soil or sand. Reduces systemic inflammation, improves sleep, lowers cortisol. Free and underestimated.
- Daily outdoor walk — even 20 minutes. Exposure to natural light and outdoor environment has documented effects on cortisol and mood.
Stress management & cortisol
The nervous system needs active tools
- Cardiac coherence — 5 minutes, 3 times per day. 5 seconds in, 5 seconds out. The simplest and best-documented tool for rapidly reducing cortisol.
- Less prolonged cardio, more strength training — prolonged cardio raises cortisol. Strength training does too, but the anabolic hormonal response that follows outweighs it. Maximum 40 minutes per session.
- Active social and intimate life — social connection reduces cortisol and stress hormones. Not optional for your biochemistry — build it deliberately.
The 8 things that change everything
- What you've done in the last 10 years shows now. But it's never too late — the right habits adopted today can reverse or significantly attenuate the effects at any stage.
- Free weight strength training is your number one tool. Squat, deadlift, lunges, plus varied 3D movement and mobility. Without machines. She who lifts well, ages well.
- Eat more protein, fewer fast carbs. Insulin resistance is the key mechanism behind abdominal fat gain. It's not about calories — it's hormonal biochemistry.
- Intermittent fasting 14-16 hours is your ally, not your enemy. Post-menopause, hormones are stabilised. Fasting improves insulin, reduces visceral fat and boosts HGH. Start with 12 hours and progress.
- The pelvic floor is trainable — start now. Daily Kegels, pelvic floor awareness in every exercise. The simplest prevention against incontinence and prolapse.
- Guérande sea salt, not refined salt. Remineralisation is essential for fascial hydration, muscle function and nervous system balance.
- Bed before 11pm is not optional. In menopause, nightly repair hormones are already compromised. Every hour of deep sleep counts double.
- Cortisol is the invisible saboteur. Chronic stress + elevated cortisol = abdominal fat + muscle breakdown + poor sleep. Cardiac coherence, earthing, active social life — these are not luxuries. They're hormonal tools.
Menopause isn't the end of something. It's the beginning of a more conscious relationship with your body.
Frequently asked questions
Does menopause permanently affect athletic performance?
No — menopausal women who train with free weights maintain levels of strength, balance and body composition comparable to active premenopausal women. Studies from 2024-2025 confirm that hormonal decline doesn't prevent training adaptations. Progress is possible at any age — it simply requires more recovery time and an adapted approach.
Do I need to consult a doctor before starting strength training in menopause?
If you have cardiovascular history, severe osteoporosis or advanced prolapse, a prior consultation is recommended. For a woman in good general health, starting with light to moderate loads under supervision of a competent coach is completely safe and strongly recommended.
Do pelvic floor exercises alone resolve incontinence?
For mild to moderate incontinence, Kegel exercises have a proven efficacy rate, particularly in women under 60. For more advanced cases or if incontinence persists after 8-12 weeks of exercise, consultation with a pelvic floor physiotherapist is strongly advised.
Is hormone replacement therapy (HRT) necessary?
HRT is a valid medical option for some women with severe symptoms, to discuss with a gynaecologist. What's documented independently: women who combine regular exercise, adapted nutrition and quality sleep show significantly attenuated symptoms — with or without HRT. Habits don't replace medical advice, but they make a real and measurable difference.